

Updates about the Pandemic Treaty being negotiated between Health Canada and the WHO, full Report
by Dan Fournier, published Monday, May 6, 12:35 EDT on fournier.substack.com

Author Note: This is not an opinion piece, but rather a news article which provides the most factual up-to-date information surrounding the WHO’s Pandemic Treaty and amendments to the International Health Regulations.
This article is segmented as follows:
3. Matters of Contention & Country Pushback
3.1 Main Matters of Contention
Financial Costs, Vaccine Passports, Contact-Tracing, Quarantine, Surveillance & Narrative Control, Loss of Sovereignty
3.1.4 WHO’s Global Digital Health Certification Network (GDHCN)
1. Introduction to the WHO and its Pandemic Treaty
According to author and researcher James Rogusky, two proposals would transform the World Health Organization (WHO) from an advisory body to a global governing body whose policies would be legally binding.
The two proposals consist of:
A treaty is formal agreement between two or more countries.
WHO Member States will convene later this month to vote on the two proposals during the 77th edition of the World Health Assembly in Geneva, Switzerland.
1.1 What is the WHO?
Since the Covid-19 Pandemic emerged in late 2019 and early 2020, billions around the globe have become more familiar with the World Health Organization, often referred to and abbreviated as the WHO.
As per their About page, the WHO is a United Nations agency that was founded in 1948.
“WHO leads global efforts to expand universal health coverage. We direct and coordinate the world’s response to health emergencies.”
1.2 Who funds the WHO?
The WHO receives its funding from two main sources: Member States paying their assessed contributions (countries’ membership dues), and voluntary contributions from Member States and other partners.
The two largest source of funds obtained by the WHO come from its top two contributing country members, the United States and Germany, along with the Bill & Melinda Gates Foundation and its affiliated Gavi [Vaccine] Alliance which was set up by the Bill & Melinda Gates foundation in 1999 with seed money of US$750 million.
Here are their respective contributions for the two last reported periods, 2021 and 2022 (Schedule 2 – Voluntary contributions for the General Fund):
2021:
US$605,088,277 from Germany
US$375,597,694 from the Bill & Melinda Gates Foundation
US$352,560,823 from the United States
US$244,540,452 from the Gavi Alliance
2022:
US$739,315,812 from the United States
US$597,344,713 from Germany
US$390,349,552 from the Bill & Melinda Gates Foundation
US$202,606,585 from the Gavi Alliance
Gavi The Vaccine Alliance’s top funders include the Bill & Melinda Gates Foundation, the United Kingdom, the United States, Norway, Germany, France, and Canada. Annual contributions and pledges can be viewed in their December 31, 2023 report.
1.3 Key Criticisms
Some key criticism have emerged since the Covid-19 Pandemic with regards to some of these key supranational organisations such as the WHO, its parent in the United Nations, and Gavi.
Gavi enjoys privileges and total immunity from prosecution, as per its agreement with the Swiss state since its headquarters are based in Geneva, Switzerland. This means that it cannot be sued for any damages resulting from its operations and recommendations of health-related guidelines and treatments, including the administration of vaccines.
Similar privileges and immunities are enjoyed by the United Nations and the World Health Organization, both with headquarters located in the Swiss capital.
Such privileges and immunities from prosecution along with the fact that Directors and heads of these international organisations are appointed rather than elected have been points of contention regarding their authority, legitimacy, and underlying motives.
Concerns about profit incentives by the WHO and Gavi’s partners in the pharmaceutical industry have also been an issue of contention, particularly given that the International Federation of Pharmaceutical Manufacturers & Associations (IFPMA) has a seat on the Gavi Board.
The IFPMA represents more than 55 members of national industry associations, including pharmaceutical giants Johnson & Johnson, GlaxoSmithKline, Merck & Co., Novartis, Sanofi Pasteur, and Pfizer.
Accordingly, there are concerns about possible conflicts of interests as well as profiteering from pro-vaccination policies and the like.
For instance, Dr. Tess Lawrie from the World Council for Health, emphasised that the WHO wants to introduce 500 new vaccines by 2030 in their Immunization Agenda 2030 (IA2030) program (see also Immunization Agenda 2030).
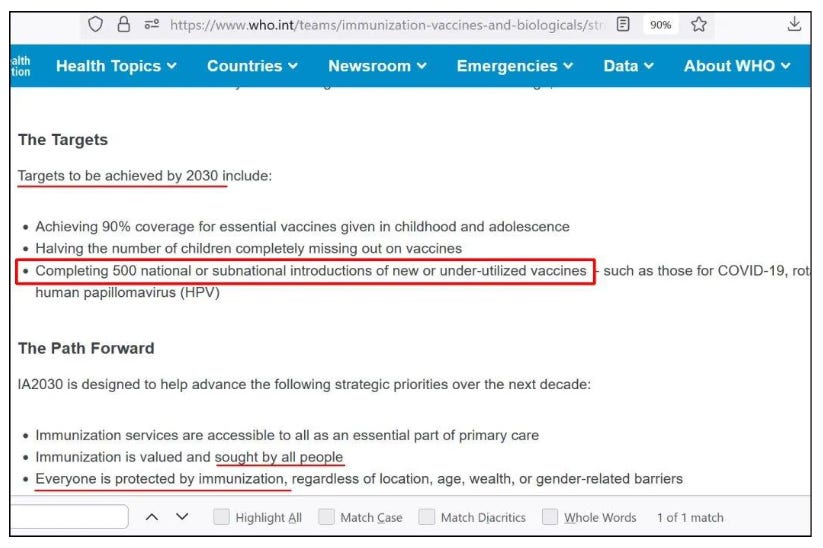
This certainly benefits pharmaceutical companies who will be producing and selling these vaccines.
2. The WHO’s Pandemic Treaty, IHRs, & INB
2.1 WHO Pandemic Treaty
In December of 2021, 194 World Health Organization (WHO) and its Member States, including Canada, agreed to launch an intergovernmental negotiating body (see section 2.4 below) to develop a Pandemic Agreement.
Many names and acronyms get thrown around which confuses the situation.
For the WHO’s Pandemic Treaty itself, the agreement being negotiated goes by many names such as:
World Health Organization (WHO) Convention
Pandemic Treaty
Pandemic Agreement
Pandemic Instrument
Pandemic Accord
It is unclear why it goes by so many names. One explanation lies with how treaties in United States are adopted, i.e., they require the advice and consent of the Senate. Regardless, any of these terms are used to refer to the same international agreement.
The WHO’s Q&A page titled Pandemic prevention, preparedness and response accord provides a broad summary of the ambitious international endeavour:
“Member States of the World Health Organization have agreed to a global process to draft and negotiate a convention, agreement or other international instrument under the Constitution of the World Health Organization to strengthen pandemic prevention, preparedness and response.”

The page shown above clarifies what is meant by a convention, agreement or other international instrument [with emphasis added]:
“Conventions, framework agreements and treaties are all examples of international instruments, which are legal agreements made between countries that are binding.
...
A key international instrument on international health, rooted in the WHO Constitution, is the International Health Regulations (2005), which was established “to prevent, protect against, control and provide a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade.”
Note from the passages above the mention of legally binding agreements.
On the same page, the WHO answers the question What is the process underway to draft and negotiate the accord? With an embedded video which can be viewed hereunder:
It also emphasises that the general public can be kept informed of the process through the International Negotiating Body (INB). See Section 2.4 below for more information about the INB.
2.2 International Health Regulations (IHR)
First, a brief backgrounder on International Health Regulations (IHR).
According to Wikipedia, the International Health Regulations (IHR) first adopted by the World Health Assembly in 1969 and last revised in 2005, are legally binding rules that only apply to the WHO that is an instrument that aims for international collaboration "to prevent, protect against, control, and provide a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks and that avoid unnecessary interference with international traffic and trade."
The entry adds: “The IHR is the only international legal treaty with the responsibility of empowering the World Health Organization (WHO) to act as the main global surveillance system.”
The latest, third edition of IHR dates from 2005 which provides the following Overview:
“The International Health Regulations (2005) (IHR) provide an overarching legal framework that defines countries’ rights and obligations in handling public health events and emergencies that have the potential to cross borders. The IHR are an instrument of international law that is legally-binding on 196 countries, including the 194 WHO Member States.”
How countries’ “rights and obligations” as well as how the instrument is “legally-binding” is the subject of interpretation and debate; and is thus beyond the scope of this article.
What is important to focus on here, though, is the current draft text of the proposed amendments to the IHR. The latest version of the document is that which surfaced from a 22-26 April 2024 meeting titled Working Group on Amendments to the International Health Regulations (2005) (WGIHR) dated April 17, 2024. Click the link for the full text of the proposed Amendments to the IHR.
The previous version was from 13 March, 2024.
2.3 Canada’s IHR Focal Point
With regards to the implementation of IHR, the Public Health Agency of Canada (PHAC) – also commonly referred to as Health Canada – states that each country is required "to designate or establish a National IHR Focal Point (NFP) and the authorities responsible within its respective jurisdiction for the implementation of health measures under these Regulations" (IHR Article 4).
Canada meets its obligations under the IHR through the following activities:
monitoring and evaluation
real-life events
emergency preparedness and response exercises
“The IHR aim to prevent, protect against, control and respond to the international spread of disease and other public health risks, while avoiding unnecessary interference with international traffic and trade. They're also designed to reduce the risk of diseases spreading at international airports, ports and ground crossings.”
Moreover, it has efforts (collaboration) between federal departments and with provincial and territorial partners; further stating that it implements the IHR under existing legislation, regulations, policies and agreements in place at both the federal and provincial/territorial levels.
Of course, each province or territory has its own laws and regulations with regards to health and emergency preparedness and response procedures. But Canada’s National IHR Focal Point notes the following on the matter:
“Because legislation differs among federal and provincial/territorial governments, Canada has mechanisms, agreements and plans in place that enable national coordination. This is particularly important during public health emergencies that require federal involvement.”
With regards to Assessment and Reporting of IHR, the National IHR Focal Point aims to “identify a potential public health emergency of international concern.” These are assessed using the IHR Annex 2 decision instrument.
The process of Assessment and Reporting in Canada also includes the following statement [with emphasis added]:
“The responsibility for determining if an event is a public health emergency of international concern lies with WHO's Director-General. This person is advised by a committee of experts (IHR Emergency Committee), who follow the criteria and procedures set out in the Regulations.”
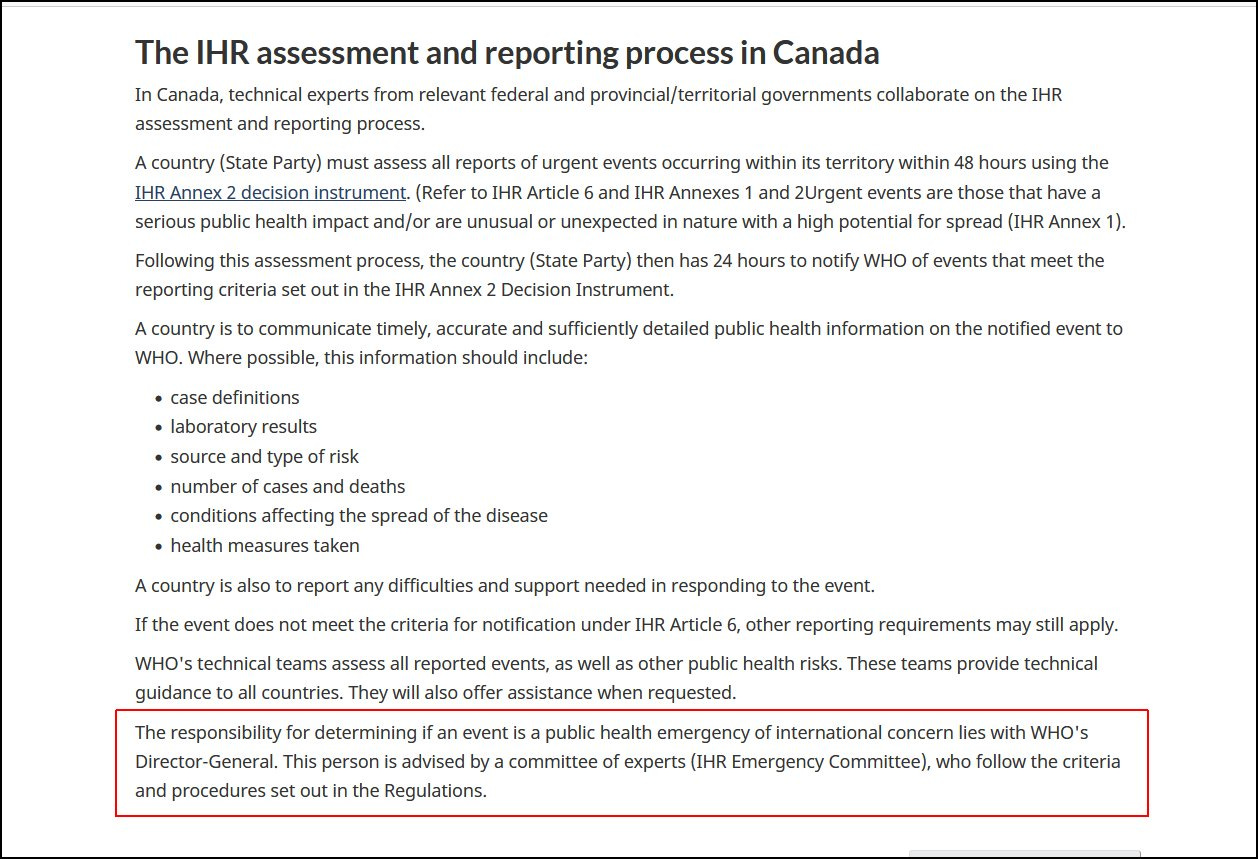
This affirms that it is the WHO Director General, currently Tedros Adhanom Ghebreyesus who can determine and declare an event as a public health emergency of international concern.
As current IHR Amendments are being negotiated, in October of 2023, I made an Access to Information (ATI) request inquiring about the communications relating to the proposed Amendments (to the IHR) that have been submitted by Canada and the WHO. Here is the text of my original request:

But after a lengthy, five month, process of being told to modify my request so as to not make the results too voluminous, I settled on the following text:
“Documents and/or communications between the Canadian 'National Focal Points' and Public Health Agency of Canada with the WHO (IHR) with regards to the following specific items:
- Vaccines - new or proposed procedures and rules for administering vaccines in the event of a future outbreaks of an international nature and any mention of "vaccine passports" for any of these.
- Disease X - any communications, documents, provisions, rules pertaining to the preparedness or response to this disease.
Starting from October 1, 2022 until the present day (January 19, 2024)”
I received the following response letter last month (April, 2024):
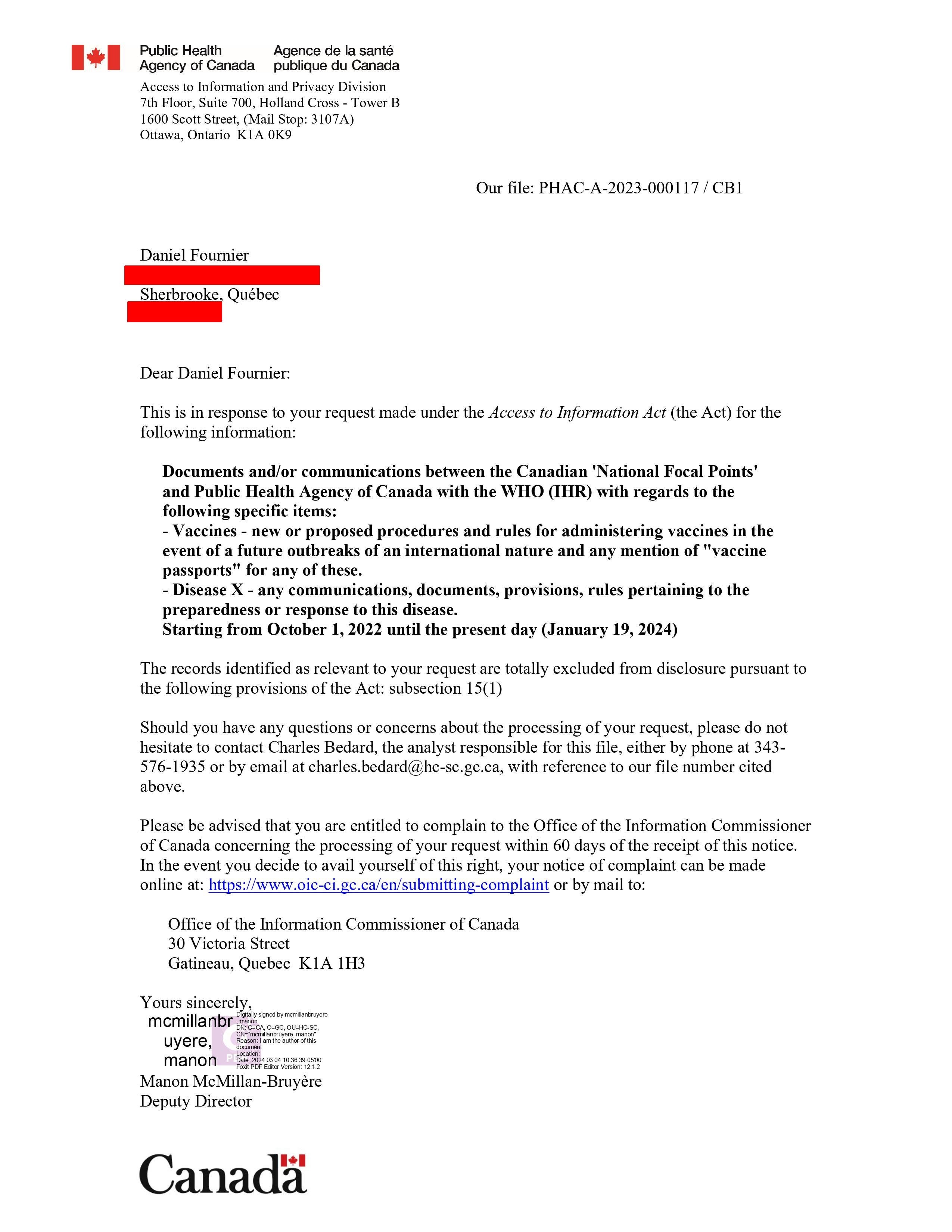
The ATI request rendered zero pages; for, the records identified as relevant to my request are “totally excluded from disclosure pursuant to the following provisions of the Act: subsection 15(1),” which can be viewed hereunder:

Put simply, all communications between Canada Public Health Agency (PHAC)’s IHR Focal Point and the WHO are strictly confidential.
2.4 Intergovernmental Negotiating Body (INB)
In December of 2021, the World Health Assembly established the Intergovernmental Negotiating Body (INB) (see https://inb.who.int) to draft and negotiate the WHO convention (Pandemic Treaty).
“The INB’s work is based on the principles of inclusiveness, transparency, efficiency, Member State leadership and consensus,” states the home page for the INB.
Two rounds of Public hearings regarding the new international instrument on pandemic prevention, preparedness and response were conducted. Here are the links along with selected video testimonies from Canadians.
First round of public hearings (12-13 April 2022)
Second round of public hearings (29-30 September 2022)
The INB process occurs in stages, with the notable submission of its final outcome to the 77th edition of the World Health Assembly in Geneva, Switzerland in May of 2024.
3. Matters of Contention & Country Pushback
3.1 Main Matters of Contention
3.1.1 Internationally
3.1.1.1 Financial Costs
On area of contention which many countries share with regards to an International Pandemic Treaty includes the associated financial costs member countries must bear.
According to a RealClearWire report, costs borne by lower income countries for the Pandemic Preparedness and Response (PPR) could be as high as $31 billion per year.
As per a medRxiv study, such high amounts would be particularly burdensome on low- to middle-income countries. Here are some excerpts from the study’s Abstract [with some emphasis added]:
“Background
Covid-19 has reinforced the strong health and economic case for investing in pandemic preparedness and response (PPR). The World Bank and World Health Organization (WHO) propose that low- and middle-income governments and donor countries should invest $31.1 billion each year for PPR. We analyse, based on the projected economic growth of countries between 2022 and 2027, how likely it is that low- and middle-income country governments and donors can mobilize the estimated funding.
Findings
Our analysis shows that low-income countries would need to invest on average 37%, lower-middle income countries 9%, and upper-middle income countries 1%, of their total health spending on PPR each year under the constant scenario to meet the World Bank WHO targets.”
The Conclusion of the study also noted alternative sources of PPR financing could include global taxation (e.g., on financial transactions, carbon, or airline flights), cancelling debt, and addressing illicit financial flows.
3.1.1.2 Vaccine Passports, Contact-Tracing, Quarantine
During the Covid-19 Pandemic, the quarantining of individuals in isolated and designated facilities or in their homes was a matter of great contention, as were vaccine passports and contact-tracing (usually through applications installed on individuals’ cell phones).
The current draft of the WHO Pandemic Treaty (17 April 2024) touches upon these very subjects, among others, in PART III – RECOMMENDATIONS.
Recommendations issued by WHO to States Parties with respect to persons may include the following advice [partial list]:
review travel history in affected areas;
review proof of medical examination and any laboratory analysis;
require medical examinations;
review proof of vaccination or other prophylaxis;
require vaccination or other prophylaxis;
place suspect persons under public health observation;
implement isolation and treatment where necessary of affected persons;
implement quarantine or other health measures for suspect persons;
implement tracing of contacts of suspect or affected persons;
refuse entry of suspect and affected persons;
implement exit screening and/or restrictions on persons from affected area.
As can be seen from the list above, several isolation and quarantining methods can be employed. Proof of vaccination, medical examinations may also be required for travel.
Depending on the level and intensity of their application by each respective jurisdiction, these could prevent individuals from travelling both domestically and internationally.
In addition, Member States requiring medical examinations can open up the door to a series of discriminatory measures, depending on the nature of the health crisis, not to mention violations of medical privacy and consent.
3.1.1.3 Surveillance & Narrative Control (countering misinformation and disinformation)
Another major area of contention has to do with provisions in the Pandemic Treaty that relate to surveillance and the manner in which Member States are to respond to the dissemination of information about a given health crisis, particularly in terms of how it can be labelled as disinformation and misinformation. These were major challenges experienced during the Covid-19 Pandemic.
In the previous version (13 March 2024) of the Revised draft of the negotiating text of the WHO Pandemic Agreement, Article 18 (see page 20) dealt with these issues.
But the newer, longer, version (17 April 2024, Working Group on Amendments to the International Health Regulations (2005) (WGIHR)) deals with these issues in the section ‘A. CORE CAPACITIES REQUIREMENTS FOR PREVENTION, SURVEILLANCE, PREPAREDNESS AND RESPONSE’ (see pp. 45-46), as is partially shown hereunder:

In short, the text compels Member States to develop mechanisms of surveillance and countering misinformation and disinformation, presumably that which is disseminated on social media platforms.
The imposition of surveillance systems can represent infringements upon individuals’ privacy rights, and is thus a major matter of contention.
As for countering misinformation and disinformation, these will prove to be very subjective, as has been and continues to be the case surrounding information related to the Covid-19 Pandemic.
And mechanisms for controlling information will vary from one jurisdiction to another, given each one’s respective laws and rights related to freedom of expression.
3.1.1.4 Loss of Sovereignty
Loss of nations’ sovereignty also figures among the most salient contentions of the Pandemic Treaty.
When talking about the Pandemic Agreement, WHO Director, Tedros Adhanom Ghebreyesus has been criticised for saying that national interests should not come in the way of global interests:
"This is a common global interest. And national interests, very narrow national interests should not come into the way."
Though worries about the World Health Organization gaining total control over Member States is neither feasible nor likely, individuals and even politicians across the globe are sounding alarm bells.
Countries vary tremendously with regards to their health approaches, health care systems and infrastructure, rights and freedoms, and so on. Therefore, no two countries will share completely views on how they wish to respond to health crises such as pandemics.
Last month, tens of thousands of people gathered in Tokyo, Japan to protest the World Health Organization’s (WHO) proposed Pandemic Treaty and amendments to the International Health Regulations (IHR). Other estimates for the rally figure as high as 100,000 participants.
3.1.2 In the United States
Author note: this subsection has been added on 2024-05-09 to insert the ReclaimTheNet.org article concerning the GOP Senators’ letter to President Biden (see the latter part of this subsection).
Some states, like Louisiana are not taking chances. As per a Need to Know news article dated April 8, 2024, the Bayoo state has passed legislation (Senate Bill 113) which prohibits the World Health Organization from exerting any kind of power within its territory and on its residents. And the same goes for the United Nations and the World Economic Forum (WEF).The bill passed unanimously (37 Yeas, 0 Nays) in the Louisiana Senate.
The text of the bill is relatively short:

The Oklahoma House passed bill SB426 denying jurisdiction in the state to WHO, UN and the WEF; here is an excerpt from the BILL SUMMARY:
“The floor substitute to SB 426 prohibits the State of Oklahoma from enforcing any mandates or recommendations by the World Health Organization, the United Nations, or the World Economic Forum including those that relate to masks, vaccines, medical testing, or gathering any public or private information about Oklahoma residents.”
Utah and Florida also have related legislation:
Utah State Legislature – S.B. 57 Utah Constitutional Sovereignty Act
The Florida Senate – CS/SB 252: Protection from Discrimination Based on Health Care Choices
Other states also have similar proposed (or pending) legislation, including:
Georgia General Assembly, SR634
Idaho Legislature, Senate Bill 1287
Iowa Legislature, House File 507
Kentucky General Assembly, House Joint Resolution 44
Michigan Legislature, House Bill 4859 of 2023
New Hampshire Legislature, House Bill 1156
New Jersey Legislature, Bill AR29
South Carolina Legislature, S0868
Wyoming Legislature, HB0091
[hereunder, added on 2024-05-9:]
On a national level, ReclaimTheNet.org has recently been reported that 49 GOP Senators Confront Biden With a Bold Plea To Halt WHO Pandemic Proposals.
They include a link to the U.S Senate letter addressed to President Biden (click for the PDF).
Here are some key excerpts from the article:
The Biden administration has thrown its support behind these proposals, which would see global health officials granted extensive control over the management of pandemics. However, the senators—all members of the Senate Republican Conference—argue that the WHO must first address its failures during the COVID-19 crisis, which, according to them, were both total and predictable. They believe these failures have caused significant damage to the United States.
Their letter emphasizes that no treaty should be signed nor amendments to the IHR approved without rectifying these shortcomings, which, if unaddressed, would potentially lead to increased authority for the WHO, undermine intellectual property rights, and endanger free speech.
The article also highlights how Senators are concerned about the lack of transparency involved with the proposed Amendments of the IHR, overall secrecy by the WHO, and its “grave threat to US sovereignty”:
Moreover, they pointed out a procedural concern: Article 55 of the IHR stipulates that any proposed amendment must be communicated to member states four months before the World Health Assembly. Yet, with the meeting fast approaching, the final text of these proposals remains undisclosed to WHO member states. This lack of transparency is alarming to the senators because some of the 300 proposed amendments could dramatically boost the WHO’s emergency powers, representing a grave threat to US sovereignty. Consequently, they declared, “Amendments are not in order.”
The 49 Senators who signed the letter also cautioned the President that if he ignores their advice, they will consider the agreement as a treaty which would thus require a two-thirds vote of the Senate under Article II Section 2 of the Constitution.
As mentioned in this article, this is likely a reason why the pandemic agreement goes by multiple names. If it is not considered a treaty, then the two-thirds rule would be irrelevant.
3.1.3 In Canada
Canadians share many of the same concerns that were listed in the previous section.
Responding to a media inquiry, Senior Media Relations Advisor Anna Maddison (from Public Affairs Branch which serves Health Canada and the Public Health Agency of Canada) mentions three common themes received by Canadians who have penned letters to authorities on the Pandemic Treaty with the WHO:
concerns around sovereignty;
ensuring that Canadian values and priorities are included in the Pandemic Agreement;
inquiring about the role of the World Health Organization (WHO) in Canada.
See Section 5.1 below for more details about these letters.
“With nations converging at the World Health Organization (WHO) this May to vote on a legally binding treaty that will transform the global regime for responding to global health emergencies, there has never been a more vital time for Canadians to be aware of what is happening at the WHO.”
The above quote is from Canadian Member of Parliament, Dr. Leslyn Lewis from a March 2, 2024 post on her Substack which also touches upon the issue of sovereignty, among other things.
“The [pandemic] treaty will be legally binding, meaning it will become a violation of international law should any nation choose to go against the WHO’s directives,” the seasoned lawyer added as an apparent warning to the passage of the proposed treaty.
“While the WHO states that it will respect national sovereignty, the reality is that this treaty will legally compel action based on decisions that are made by unelected WHO technocrats when a public health emergency of international concern (PHEIC) is declared,” the Canadian lawmaker added.
In her post, Lewis also mentioned that Canadians are concerned about the suspension of Charter rights as was the case during the Covid-19 Pandemic.
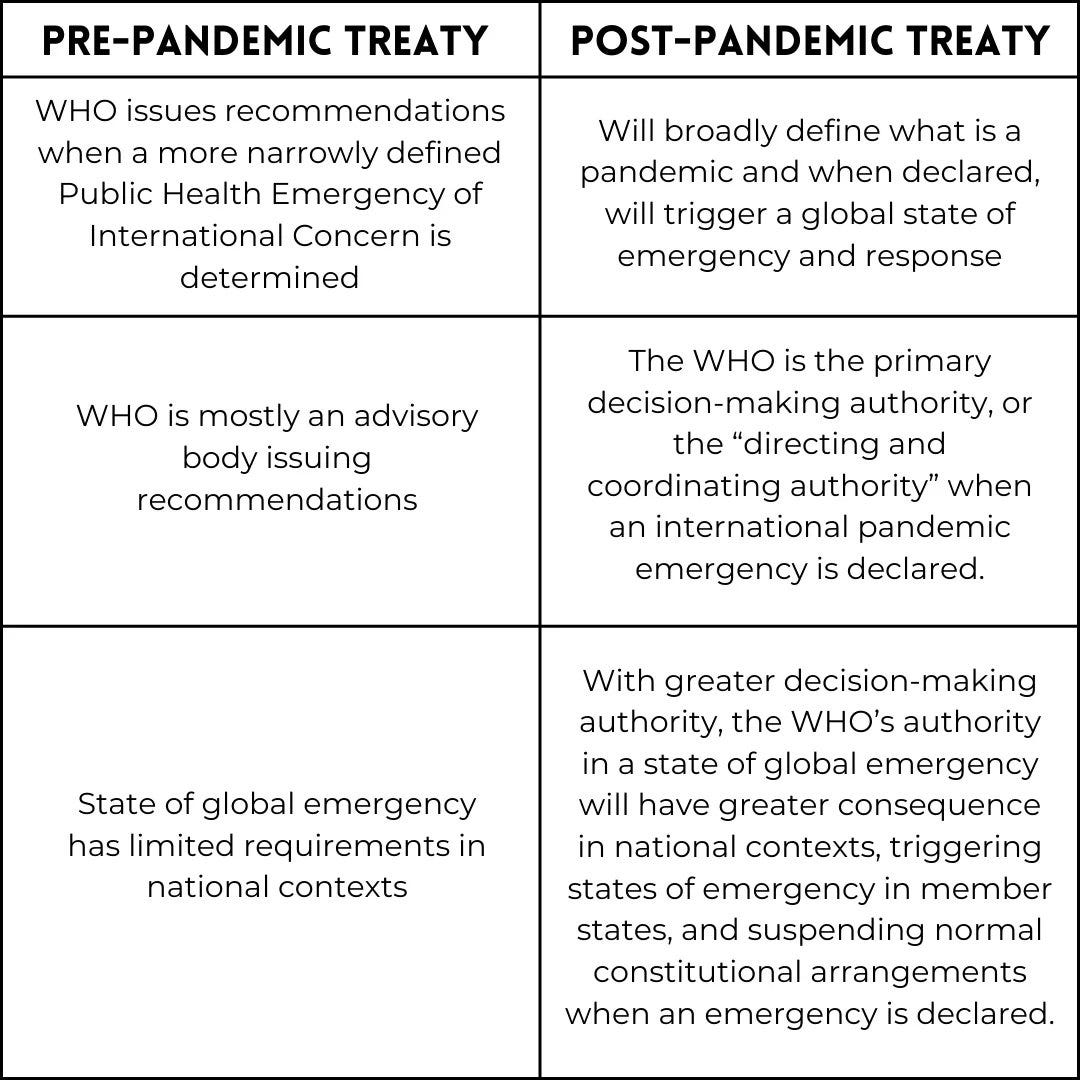
She also cautioned that the manner in which pandemics and PHEICs are dealt with will change once the once the Pandemic Treaty is approved.
Lewis provided a table that compares the “PRE-PANDEMIC TREATY” with a “POST-PANDEMIC TREATY” scenario:
Apart from her criticisms towards the “WHO technocrats,” Parliamentarian Dr. Leslyn Lewis is also no fan of its parent organisation in the United Nations since she presented a petition to the House of Commons calling upon the legislative body to “urgently implement Canada's expeditious withdrawal from the UN and all of its subsidiary organizations, including WHO.”
In the Canadian province of Quebec, Réinfo Québec – an an arm of an international collective of 4,000 doctors and 80,000 members – also weighed in on the Pandemic Treaty, stating that it would hinge upon rights and freedoms of citizens. They also produced a brochure and invited citizens to send a letter to the provincial Public Health Minister, Dr. Luc Boileau, outlining the various pitfalls of the treaty.
3.1.4 WHO’s Global Digital Health Certification Network (GDHCN)
Two other major areas of contention individuals have has to do with the sharing of their private medical information and their vaccination status.
As per the WHO’s Global Digital Health Certification Network (GDHCN) initiative, this network may include the following (taken verbatim from their page):
the digitisation of the International Certificate of Vaccination or Prophylaxis,
verification of prescriptions across borders,
the International Patient Summary,
verification of vaccination certificates within and across borders,
certification of public health professionals (through WHO Academy).
Should all of the above data and information be collected by the GDHCN, it would be comprised of a great deal of personal private medical information of citizens from around the world, likely stored in a centralised hub which could also entail possible security breaches.
This also leaves the determination of who exactly would get to determine the rules and restrictions for travel across country borders, in addition to the continuously changing dynamics and complexities that usually surround pandemics or other health emergencies.
Moreover, refusal of travel could open up a whole set of issues with regards to mobility rights, access to public services, and discrimination – which also vary from one jurisdiction to another.
To meet this need, in line with the Global strategy on digital health priority actions (2020-2025), the WHO has established the Global Digital Health Certification Network (GDHCN).
The GDHCN network is modelled and built upon the experience of regional networks for COVID-19 Certificates as per the previous, very unpopular, European Union Digital COVID Certificate (EU DCC) system that had been approved and implemented by the European Commission during the Covid-19 Pandemic.
Importantly, the network would be operationalised through a software infrastructure platform that enables Member States to bilaterally verify the authenticity of digital records and health certificates through an interoperable trust architecture, without WHO participating in any verification processes but acting as a “trust anchor.”
It is unclear what is meant by “trust anchor.”

Expanding on the previous European model, the WHO is also thinking ahead in that it seeks to use a staged approach to cover additional “use cases,” though these are not yet defined.
“Expanding such digital solutions will be essential to deliver better health for citizens across the globe,” the related news release notes.
Here too, by using the term “expanding,” the WHO is implying that additional measures will be added in the future to their “digital solutions.” It remains unclear who will determine which additional measures get added.
“With this collaboration, WHO will facilitate this process globally under its own structure with the aim to allow the world to benefit from convergence of digital certificates,” the release also confirms.
Though it is written that it is a “collaboration,“ it still states that the process would fall “globally under its own structure” which implies that the WHO would have centralised control over the process.
Furthermore, the release indicates the establishment of a “global system that will help facilitate global mobility and protect citizens across the world from on-going and future health threats, including pandemics.”
Again, they are not defining important terms and phrases. For instance, “health threats” could encompass a very large variety of health-related issues – which can be perceived and considered differently across different countries and regions across the globe.
4. Canada’s Role & Negotiators
As per Health Canada’s Canada’s role in the development of an international pandemic agreement web page, Canada is working closely with other countries and international partners to “strengthen global pandemic prevention, preparedness and response.”
4.1 Zoe Khan, Chief Negotiator for the WHO Pandemic Agreement
Zoe Kahn works as Chief Negotiator with regards to the Pandemic Treaty for the Public Health Agency of Canada.
“Bold action is needed to ensure that we’re better prepared for the next pandemic,” stated Mrs. Khan during a WHO Pandemic Accord discussion last September.
As per a reply from Mrs. Khan that has been forwarded to this author by the receiver, the Chief Negotiator stated [with emphasis added]:
“Canada is a strong supporter of the WHO and engages with the WHO to advance domestic and development health priorities, share Canadian expertise on health issues, and protect the health of Canadians and people around the world. Our continued commitment to the WHO includes our interest in making it a strong, accountable, and well-governed institution.
…
Protecting the health and safety of all Canadians is a top priority of the Government of Canada. COVID-19 has demonstrated the need to take bold action to ensure we are better prepared for the next pandemic, which is why Canada is working closely with international partners, including the WHO, the Pan-American Health Organization (PAHO) and the global community to strengthen global pandemic prevention, preparedness and response.
The team responsible for negotiating the Pandemic Agreement is made up of representatives from the Public Health Agency of Canada/Health Canada’s Office of International Affairs for the Health Portfolio, as well as representatives from Global Affairs Canada and the Permanent Mission of Canada to the United Nations in Geneva.
When negotiating a new international agreement such as the Pandemic Agreement, the Government of Canada will always carefully consider its potential impact on our domestic laws and policies, and if there is a need for a domestic legislation to implement our international obligations. As the WHO does not have jurisdiction in Canada, Canada will remain in control of any future domestic decisions about national restrictions or other measures related to pandemics.
The Pandemic Agreement continues to be discussed by the Intergovernmental Negotiating Body and you can read about the latest updates on their work at the following website: https://inb.who.int/.”
4.2 Pandemic Agreement Team
In her reply from above, Mrs. Khan made reference to a team responsible for negotiating the Pandemic Agreement.
“Due to privacy considerations, we are unable to provide a list of staff names,” was the reply I received to an inquiring asking for the names of the members of the Pandemic Agreement Team.
Members of Pandemic Agreement Team are comprised of individuals from the following three organisations:
Public Health Agency of Canada (PHAC);
Global Affairs Canada;
Permanent Mission of Canada to the United Nations in Geneva.
As public servants acting on behalf of official government institutions, such disclosures should be made public, but are not.
A follow-up inquiry has been made regarding this matter; should an answer be forthcoming, it will be added to this post.
4.3 Permanent Mission of Canada to the United Nations in Geneva
Health Canada also refused to disclose the name of the members of the Permanent Mission of Canada to the United Nations in Geneva.
Members of this Permanent Mission are currently unknown.
5. Transparency
5.1 Canada’s Engagement with “Partners” & “Stakeholders”
Health Canada states that it is taking a “whole-of-government, whole-of-society” approach in the development of the Pandemic Agreement to “ensure that Canadian priorities and values are reflected,” adding:
“Canada’s engagement strategy aims to facilitate meaningful and inclusive engagement with partners and stakeholders. These include:
youth
private sector
academic experts
Indigenous organizations
civil society organizations
provincial and territorial governments”
They also point to an August, 2023 publication titled Pandemic Instrument Partner and Stakeholder Engagement Forum from feedback collected on March 21 and 22, 2023 which had welcomed 94 in-person participants in Ottawa and an additional 70 online participants.
Moreover, from a response received to my media inquiry, attendees represented at this forum consisted of academic experts and researchers (27%), non-governmental organisations and not-for-profits (28%), health and allied health services (14%), the private sector (13%), provincial, territorial, and Indigenous departments of health and health authorities (12%), and youth (6%).
Health Canada also confirmed that from January 29 to February 12, 2024, the Government of Canada hosted the Pandemic Agreement Regional Engagement Series which focused on gathering partner and stakeholder input on the negotiating text of the WHO Pandemic Agreement. These engagement sessions were held across various Canadian cities and included a total of 75 individuals attending in person and 41 attending online.
Thus collectively for these two consultations, we are talking about feedback obtained from at total of 280 participants.
The Senior Media Relations Advisor also confirmed that the Pandemic Agreement Team engages with Canadians through other channels such as the Health Canada Stakeholder Registry (CSIMS), social media posts (LinkedIn), and correspondence letters.
Those who signed up to CSIMS were notified of the draft negotiating text and had the opportunity to provide written comments and input to the Pandemic Agreement email address pandemicinstrument.instrumentsurlespandemies@hc-sc.gc.ca.
Lastly, the Pandemic Agreement Team receives letters that are addressed to Members of Parliament, the Minister of Health, members of the Permanent Mission of Canada to the United Nations in Geneva, as well as the Chief Negotiator of the Pandemic Agreement, Zoe Khan.
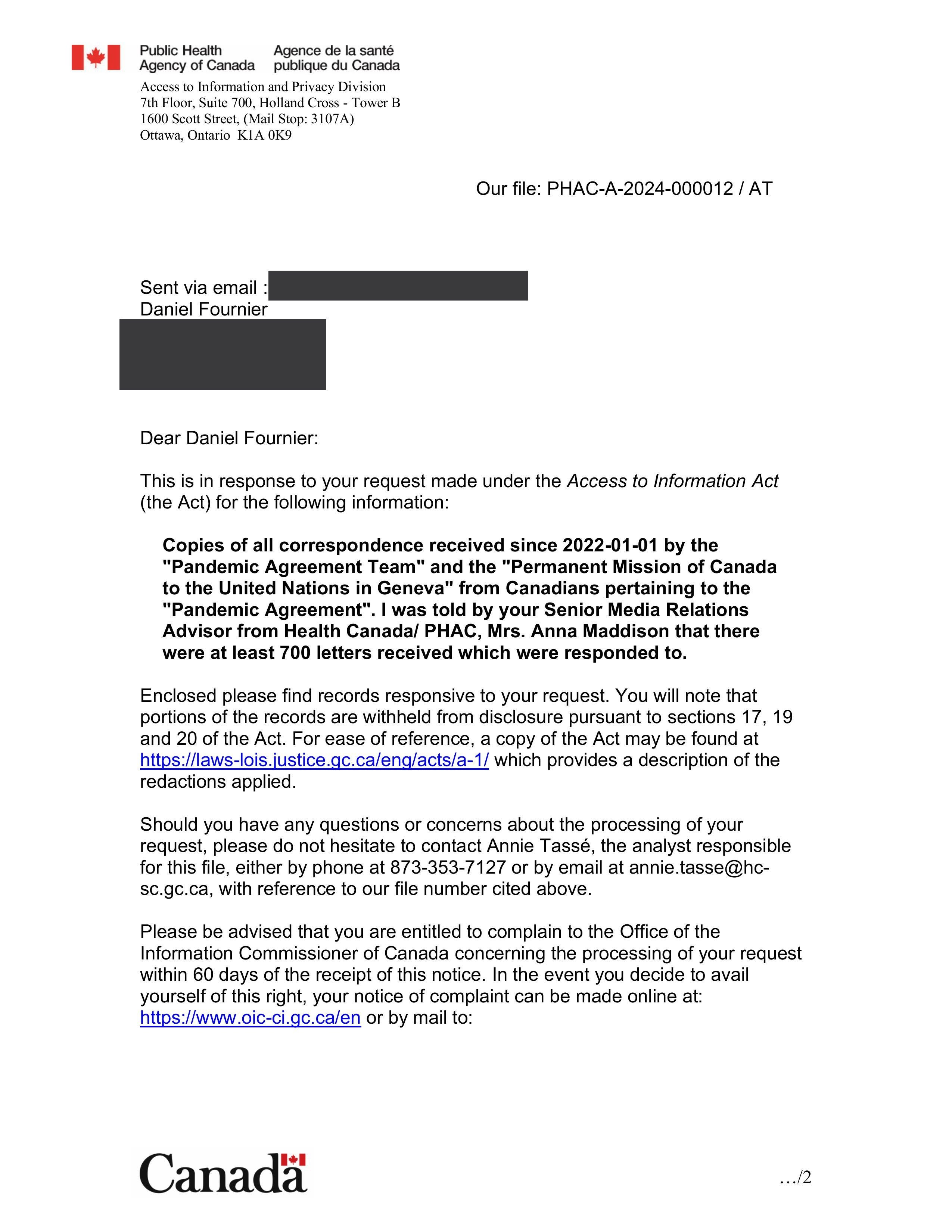
To date, the Pandemic Agreement Team and the Permanent Mission of Canada to the United Nations in Geneva have received about 700 letters and provided responses.
An Access to Information (ATI) request has been made by this author to receive copies of these letters.
[ADDENDUM 2025-01-27 BEGIN: PHAC Releases the 700 letters]
Though I received the response and release package (446 pages) by the PHAC regarding the 700 letters back in August of 2024, I am just now adding them here.
While I have not read every single letter in the large set, all of them which I have read are negative and in opposition to Canada and the PHAC joining the WHO’s Pandemic Agreement.
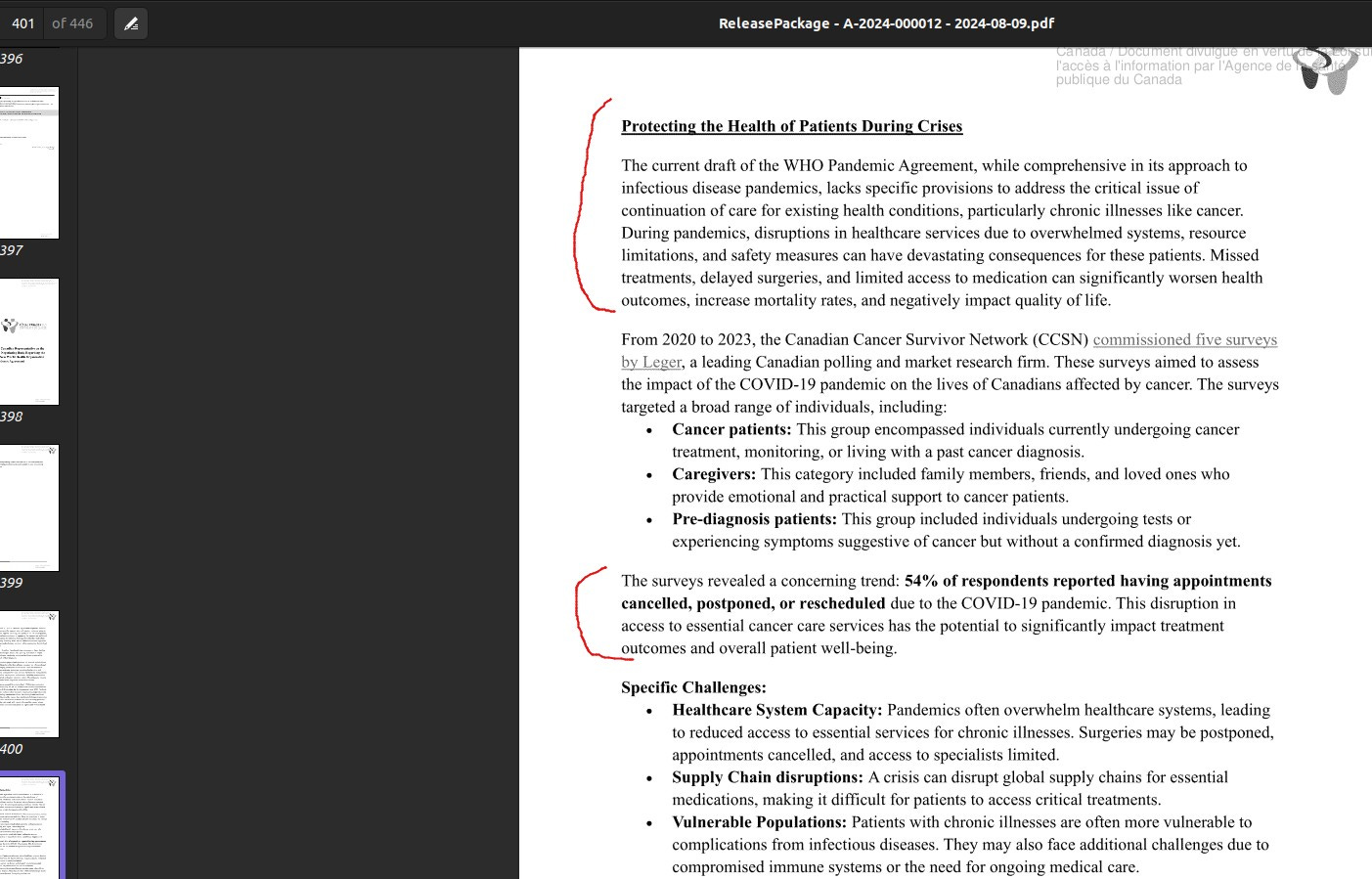
Moreover, even organisations such as the Canadian Cancer Survivor Network (CCSN) has serious issues about how pandemic are handled and how COVID-19 had very detrminental effects in this regard (see image below).
Here is the response letter I had received from PHAC back in August 2024:
And click the following image which shows the 1st of 446 pages to view the full release package which shows the scathing letters that are mostly in stark opposition to joining the WHO Pandemic Treaty.

Note that this is in the context whereby Zoe Kahn, the Public Health Agency of Canada (PHAC) Chief Negotiator for the Pandemic Treaty is still, despite this stark opposition by the Canadian populous (as shown in the letters), is continuing to negotiate to bring Canada into this Pandemic Agreement.
For more recent news (2025), consult the following resources:
James Rogusky - Hey Canada...Contact Zoe Kahn, Canada's Chief Negotiator for the Pandemic Agreement, in advance of the upcoming meetings scheduled for 17-21 February 2025 to express your opinion. (published Jan. 23, 2025), and
James Rogusky Rumble channel - PANDEMIC AGREEMENT NEGOTIATIONS - UPDATE FOR CANADA (published Jan. 24, 2025)
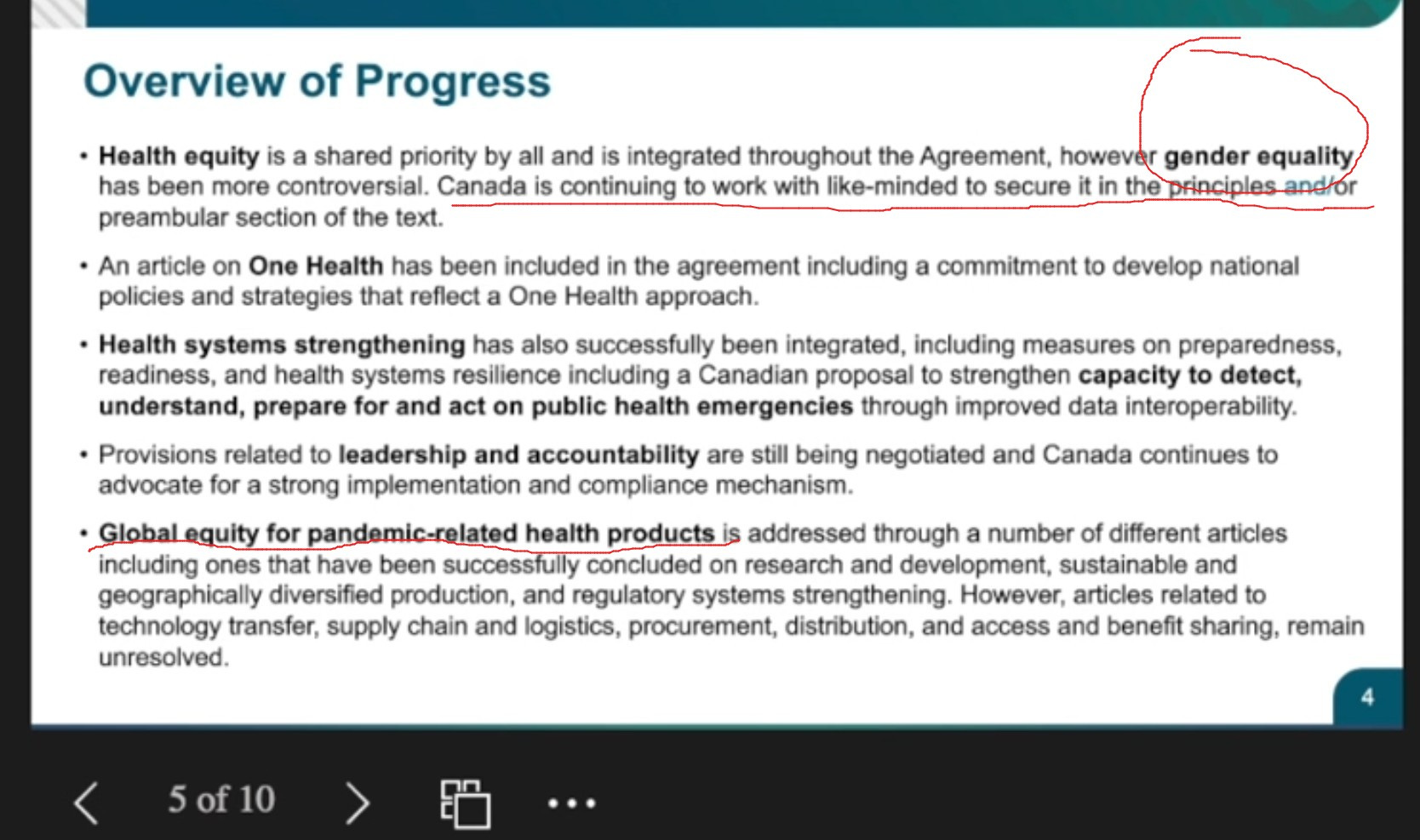
And here are a few screenshots from Zoe Kahn’s recent presentation with the first one showing how even gender equality of the woke agenda seems to be [strangely somehow] woven into this Pandemic Agreement:
The next slide from her presentation shows how the PHAC intends to possibly adopt and ratify the agreement after its May 2025 meeting at the 78th World Health Assembly (WHA):
[ADDENDUM 2025-01-27 END]
Members of the broader public are invited to share their views on the Pandemic Treaty by emailing pandemicinstrument.instrumentsurlespandemies@hc-sc.gc.ca.
6. Treaty Deadlines & Adoption, and Anticipated Delays
As is reported by The Washington Stand, all 194 WHO member nations will vote on the Pandemic Agreement at the 77th World Health Assembly from May 27-June 1 (in Geneva Switzerland).

Director-General of the WHO Tedros Adhanom Ghebreyesus attends the World Health Assembly, at the United Nations in Geneva, Switzerland, on May 21, 2023. Photo credit: REUTERS/Denis Balibouse via ThinkGlobalHealth.
Health Policy Watch, an independent global health reporting outfit, recently reported that the World Health Assembly is likely to see a basic ‘consensus’ on the Pandemic Agreement as the “hard decisions” are [likely to be] deferred.
In a separate report, they also outlined that many of the articles that deal with international co-operation will be delayed, including the ‘WHO Pathogen Access and Benefit-Sharing System’ which is commonly referred to as the PABS System (see Article 12 on page 12 of the Pandemic Treaty for more information).
Similar delays are said to be related to Research & Development whereby Parties are supposed to be collaborating on (see Article 9).
Refer back to this post in the future, for as more relevant developments become available, they will be added in the Addenda section below.
7. Addenda
7.1 Addendum - The Treaty was not agreed upon, but the Amendments to the IHR have been adopted
According to James Rogusky, The Amendments to the IHR have been adopted.
The Treaty itself was not agreed upon at the 77th edition of the World Health Assembly in Geneva, Switzerland this past May of 2024.
ABC News also reported on the failed agreement: Efforts to draft a pandemic treaty falter as countries disagree on how to respond to next emergency, May 24, 2024.
Support Independent Journalism
As an independent journalist, I take great care and pride in providing my audience with quality investigatory work and writings.
This is the kind of work that is seldom reported on in as much detail by the mainstream media, for they also tend to avoid the subjects and sometimes controversial topics that I, myself cover.
As an independent, I get paid very little for this work, for the bulk of my revenue comes from Substack subscriptions, and I am mostly surviving and supporting my family by means of personal savings.
You can support my work by considering a paid subscription to my Substack – Dan Fournier’s Inconvenient Truths (for only $5 a month, or $50 a year).
I am still waiting for a Founding Member for my Substack which could be you.
For one-time donations, you can also buy me a coffee.
If you are unable to support my work financially, it is greatly appreciated if you can share it on your social media feeds, for this brings additional exposure (and much needed eyeballs) which can lead to new paid subscribers.
Your comments are most welcome and appreciated and can be given in the Comments section below.
I sincerely thank you for your time and support.
Disclaimer:
None of what appear in this article is to be taken as medical advice.
See the author’s About page for full disclaimer.


{kind=link}

Fantastic work Dan! I really appreciate the Canadian information and the link to write and offer my opinion and concerns as a Canadian citizen on the treaty and amendments. The secrecy and lack of transparency is especially egregious. I see that Mrs. Kahn did not answer your question about this. Dr. Meryl Nass and Dr. Tess Lawrie have both brought up that a completed draft of the IHR amendments must be presented to all 193 countries 4 months in advance of the vote. The Netherlands is asking for a delay on the vote for this reason and if they can't get a delay, they will vote No. If more countries would ensure that the WHO is following their own rules by delaying the vote, that would be a start. Why the rush? Pandemics are so rare and not usually pandemics at all. Could you submit your articles to The Brownstone Institute or other venues? You are an excellent journalist and they would be lucky to have you. Thanks again Dan.
Excellent and thorough research. Thank you.